


No, Captain Tom wasn’t raising money for the NHS
No, Captain Tom wasn’t raising money for the NHS
It was for NHS Charities, and the difference matters.

Sir Captain Tom Moore has died, which is sad. He was, it appears, a nice man who ascended to hero status after going almost as viral as the pandemic during the last year of his life. Why? He walked lengths (not laps, as pedants point out) of his garden and in the end, this one simple act of charity raised £32.9m. That’s around £39m once gift aid is taken into account*. A great achievement that should be widely celebrated.
But for what cause was he raising money? According to many viral tweets over the last year and in the wake of his death, he was raising money for the NHS. An act that is damning of the government for not funding the NHS properly.


However, Captain Tom did not, in fact, raise money for the NHS.
Contrary to the emerging mythology, Captain Tom’s cash was not to pay for the ventilators and PPE used in intensive care wards. Nor was he paying the salaries of the heroic doctors and nurses working on the frontlines. The NHS is, after all, funded mostly by the government. A combination of general taxation and National Insurance.
Captain Tom was in reality raising money for a group called NHS Charities Together, which is a central node for dishing out charitable cash to reportedly around 250 smaller charities that all have links to the NHS hospitals and trusts and the like.
And because the pandemic has been dragging on for so damn long now, we in fact already know some of what Captain Tom’s money has been spent on.
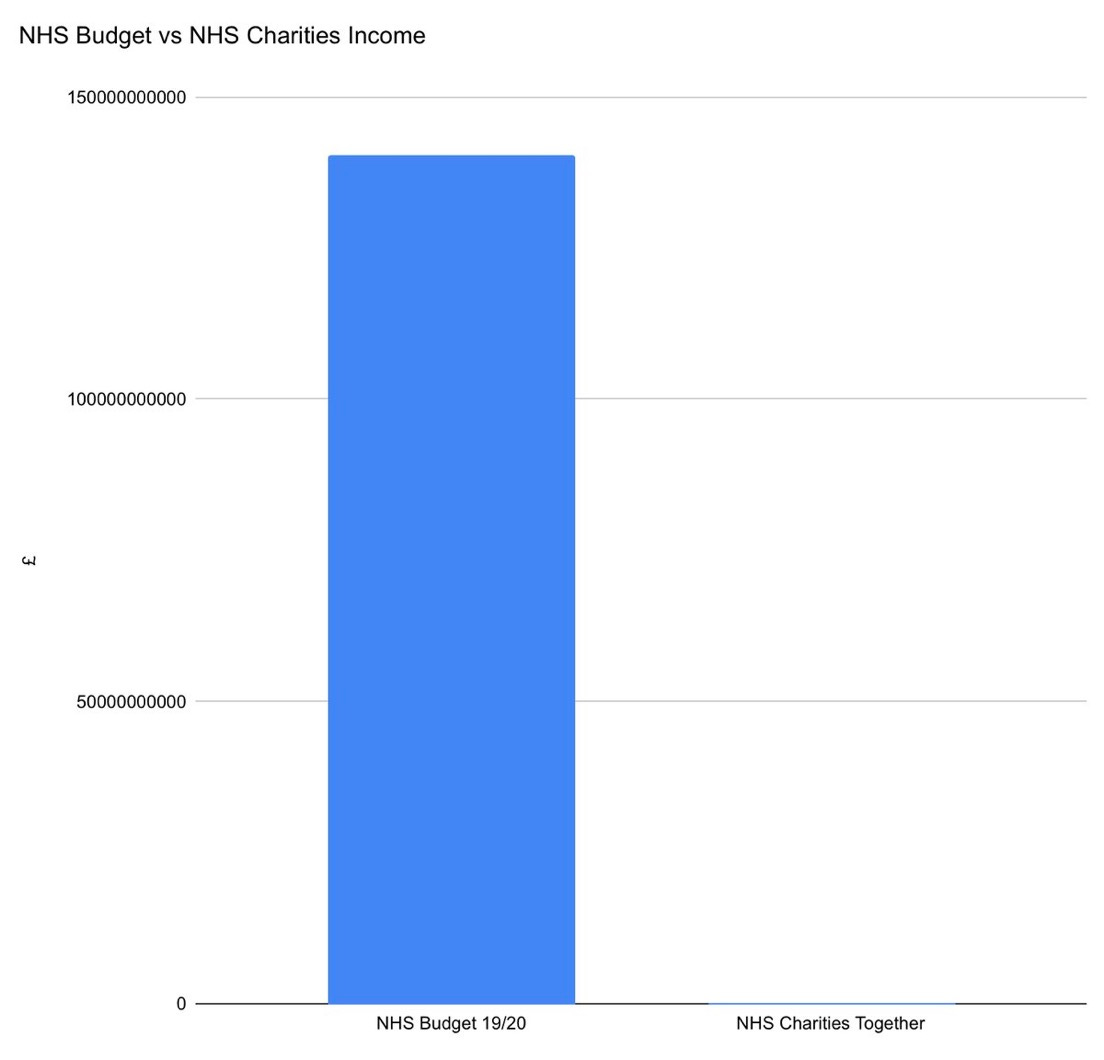
According to NHS Charities Together, its COVID-specific appeal has raised a tasty £140m, and this has been spent on things like providing NHS staff with more comfortable break areas, tablets and devices to help staff and patients stay in touch with their families, and bereavement support. Plus a whole host of other good causes, such as hospices, and specific outreach to BAME communities and people with disabilities.
In other words, Captain Tom hasn’t been funding all of the services that these tweets imply. He’s been funding things that are non-clinical***. Don’t get me wrong, having all of these extras is better than not having them, but had he raised £0 and remained a nice, but non-famous old man, the resources in hospitals and the throughput of COVID patients through Britain’s health service would be very similar.
Why be an arsehole?
So, you might wonder, why am I being an arsehole about this? Why am I picking on these viral tweets and this one specific claim, when Captain Tom’s money is still, ultimately, going to good causes? And depending on how generous you are with language, it is kind-of, sort-of, albeit not-really being spent on the NHS? Why do I hate the nice old man?
The answer is because if we don’t speak accurately, it is impossible to have a grown-up conversation about the NHS. Without understanding the complexities of health policy and government spending, we can’t make progress. All of the rah-rah platitudes in the world can’t capture the dizzying complexity of healthcare. And you don’t have to dig very deep at all to discover why actually its a bit more complicated than that.
For example, the tweet from Rachel Clarke above suggests the NHS should be “properly” funded. I agree, but what does that actually mean? The real and more important question should be: Where do we draw the line between what should be funded by taxation, and what should be funded by charity?
This is a harder question than it may appear. Obviously if something like an x-ray machine required charitable funding, that would be crazy. But what about the less essential improvements?
If we wanted, the government could use taxation to transform crumbling NHS buildings into modern, glass palaces with showpiece architecture. Or we could ensure that every patient has a Playstation 5 to pass the time while recovering, and serve caviar in the staff canteen.
The problem with healthcare in particular is that there will never be enough money. There will always be something else that can be done to improve services or improve conditions for patients. An extra diagnostic test, an extra nurse, another expensive new machine. Our needs and wants will never be satiated. This is why we have to ration healthcare services and pick and choose what is and isn’t paid for by taxation.
My own view, as a non-expert in healthcare, is that many of the things NHS Charities Together funds do sound important and like the sort of things that taxation should be funding. I am very emotionally comfortable with the idea of paying NHS staff whopping great big salaries and giving them a big bonus for their work during the pandemic. But, at some point, there will be a trade-off** and a line will have to be drawn.
This means that even if we had a more lavishly funded NHS, there would still ultimately be a role for charity at some point, and figuring out where we want that to be, instead of barking out basically meaningless slogans is probably a better use of our time.
That’s enough of that.
Anyway, that’s enough of me inadvertently shitting on Captain Tom’s mythology. I didn’t even get around to pointing out that the viral tweets are even more stupid once you compare the actual NHS budget with NHS Charities Together’s actual income. I don’t even think the column on the left takes any extra COVID cash into account.
Nor did I even get to explain how the social media discourse around public vs private in the NHS is stupid too. Maybe I’ll do another post some day.
Ultimately, the good news is that Captain Tom’s money is still going to go to plenty of good causes. And it will, slightly indirectly, help the NHS. But it is still important to be accurate, and acknowledge that no, Captain Tom wasn’t raising money to “fund the NHS” in the sense that is heavily implied by the viral tweeters.
This is my first Substack post. Would you read another? Why not subscribe and I might write another one.
(*Though I guess, amusingly, gift aid is basically a tax write-off, so claiming the gift aid is a bit like taking a chunk of cash, a proportion of which would ordinarily go to the NHS, and spending it on NHS Charities instead…)
(**As an aside, I do wonder if, in fact, funding some of the NHS Charities stuff centrally could lead to some unusual perverse incentives. Imagine, for example, the screaming Daily Mail splashes about tax payers cash being used to buy iPads and redecorate break rooms instead of being spent on employing more nurses.)
(***UPDATE: When this post was originally published instead of using the phrase “non-clinical”, I did in fact say “for lack of a more compassionate term, non-essential”. This has led to a lot of people getting mad and missing the point I am making, so I have decided to edit this for clarity. My point, however, remains the same. If only my brain could have conjured the word “clinical” when I wrote this incredibly late last night!)
(If you’ve made it this far you really should subscribe!)
I've only just read this, of course, because last year I'd never even heard of Substack, let alone Mr O'Malley. And how mad would you have been then if you had known what they were actually spending the money on! Did you ever write your piece about private v public within the NHS? It amuses me that the general public never understands that most GPs are private providers!
This is deliciously brutal.
I can sense them now. I can taste the fresh Tears of the Twitterati and bask in the deep red glow of the faces of irate gammons on Facebook who accuse me of 'disrespecting' the old trooper.
I can hear the shrill gasping of the clap-fascists and their Two Minutes Hate for anyone who dares not bow down to mindless local community obedience, as well as the future notes rustling through the hands of sulking skinflints on their way to the doctors and nurses bank accounts.
And it is glorious.